|
|
Post by jenis40 on Sept 29, 2017 14:48:35 GMT
I keep seeing estimates of how much it will cost to insure people under a single payer system, and those costs are usually along with "this is xx much higher than the current budget." But wouldn't people be paying more money in to the government under a single payer system? The money that they are currently paying towards their premiums would be going towards the new insurance (hopefully at a much lower premium cost)? I'm not good with the numbers aspect so am genuinely asking a question. Not sure if I am missing something? That's exactly how Colorado positioned it's universal care bill. Colorado's current income tax is 5% - it proposed an additional 10% payroll tax for single payer with the rationale that you would no longer be paying $10,000-15,000 for health care. It failed overwhelmingly (80% rejection). Part of that was concern with how it was combine with Medicare, a big part of it was people on private, employer plans didn't want to lose them. Another concern was that the rationale that if your employer is currently paying $12,000 in medical premiums, they would pass that on to you as higher salaries and there was a lot of concern that it wouldn't happen, and people would be left with the same salary and an additional 10% tax. I can understand why that would fail with that much 'maybe' in the proposal. Employers would have to be required to pay a percentage of the premium either directly or in salary increase. This would have to be part of the law in order to succeed. |
|
|
|
Post by #notLauren on Sept 29, 2017 14:49:07 GMT
They are also not single administrated. Show the graph for "a single admin system w/o profit - just like most developed countries" NOT a graph for universal coverage. Great. Let's follow most of the rest of the developed world into "Govt supported universal coverage". Preferably as single admin as it reduces billions in duplicative admin costs. And I'll ask again, do you pay any federal taxes? I'm not asking you to tell me your income; just whether you pay federal income tax. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 14:57:16 GMT
I keep seeing estimates of how much it will cost to insure people under a single payer system, and those costs are usually along with "this is xx much higher than the current budget." But wouldn't people be paying more money in to the government under a single payer system? The money that they are currently paying towards their premiums would be going towards the new insurance (hopefully at a much lower premium cost)? I'm not good with the numbers aspect so am genuinely asking a question. Not sure if I am missing something? This has always been my question too and I've not seen it laid out anywhere. This links to 4 different studies of Bernie Sanders Medicare for all plan and settles on an estimate of $25 trillion over 10 years: www.crfb.org/blogs/sanders-introduce-single-payer-bill-how-much-will-it-cost |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:07:30 GMT
That's exactly how Colorado positioned it's universal care bill. Colorado's current income tax is 5% - it proposed an additional 10% payroll tax for single payer with the rationale that you would no longer be paying $10,000-15,000 for health care. It failed overwhelmingly (80% rejection). Part of that was concern with how it was combine with Medicare, a big part of it was people on private, employer plans didn't want to lose them. Another concern was that the rationale that if your employer is currently paying $12,000 in medical premiums, they would pass that on to you as higher salaries and there was a lot of concern that it wouldn't happen, and people would be left with the same salary and an additional 10% tax. I can understand why that would fail with that much 'maybe' in the proposal. Employers would have to be required to pay a percentage of the premium either directly or in salary increase. This would have to be part of the law in order to succeed. It did include employers paying 1/3 of the payroll tax, or was it 2/3s? I can't remember, but one of them. I think too many people like their private insurance which is why a combo catastrophic and private might work. Many, many systems include a private insurance component. I think I read more than half of Australians have purchased complementary insurance as the universal coverage pays 100% of hospital but 75%(?) of other services so they purchase a private policy for additional coverage (perhaps one of our Australian peas can weigh in). |
|
|
|
Post by jenis40 on Sept 29, 2017 15:08:00 GMT
What I'm looking for is something that shows current insurance of $1,000 would be replaced by a single payer premium of $___. And FTR, I don't support Bernie's plan. I've always said i support single payer but what i truly support is a system closer to Germany's. A mix of state-run healthcare pools and private insurance. Everyone is covered but there is some choice. And employers are required to pay a percentage. To get there in America, I think we need to allow people to buy into Medicare/Medicaid, especially in places where there is only one insurer in the marketplace. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 15:10:19 GMT
Because it assumes the current for profit labs, hospitals, equipment, pharmaceuticals , etc. Get the Profit out,, save trillions |
|
|
|
Post by jenis40 on Sept 29, 2017 15:12:36 GMT
I can understand why that would fail with that much 'maybe' in the proposal. Employers would have to be required to pay a percentage of the premium either directly or in salary increase. This would have to be part of the law in order to succeed. It did include employers paying 1/3 of the payroll tax, or was it 2/3s? I can't remember, but one of them. I think too many people like their private insurance which is why a combo catastrophic and private might work. Many, many systems include a private insurance component. I think I read more than half of Australians have purchased complementary insurance as the universal coverage pays 100% of hospital but 75%(?) of other services so they purchase a private policy for additional coverage (perhaps one of our Australian peas can weigh in). I don't support a high deductible catastrophic plan simply because of what I personally went through. I've met my deductible & max OOP for four years now. I would be bankrupt if I had to pay $15,000 each year instead of the $4,000 I've had to pay. Private insurance that complements like Medicare Advantage, etc would be fine. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:15:18 GMT
What I'm looking for is something that shows current insurance of $1,000 would be replaced by a single payer premium of $___. And FTR, I don't support Bernie's plan. I've always said i support single payer but what i truly support is a system closer to Germany's. A mix of state-run healthcare pools and private insurance. Everyone is covered but there is some choice. And employers are required to pay a percentage. To get there in America, I think we need to allow people to buy into Medicare/Medicaid, especially in places where there is only one insurer in the marketplace. I've never see one - most of the single payers don't use premiums - they're fully financing through increased taxes. So there's a whole lot of hand waving around taxes and who's going to actual pay for it. Here's some numbers around some of the universal castrophic proposals floating around - cost to the beneficiary of $2,000 per year with the government cost less than projected ACA implementation. www.forbes.com/sites/realspin/2014/01/10/how-to-achieve-universal-health-coverage-at-half-the-cost/#7b0f8b0613dcIn general, I'm often frustrated with lack of hard data and numbers for proposals. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:16:04 GMT
Because it assumes the current for profit labs, hospitals, equipment, pharmaceuticals , etc. Get the Profit out,, save trillions Are you seriously talking about nationalizing all of the hospitals, drug companies and medical equipment manufacturers? |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 15:17:18 GMT
Because it assumes the current for profit labs, hospitals, equipment, pharmaceuticals , etc. Get the Profit out,, save trillions Are you seriously talking about nationalizing all of the hospitals, drug companies and medical equipment manufacturers? Nope. Just making them non-profit. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:20:29 GMT
It did include employers paying 1/3 of the payroll tax, or was it 2/3s? I can't remember, but one of them. I think too many people like their private insurance which is why a combo catastrophic and private might work. Many, many systems include a private insurance component. I think I read more than half of Australians have purchased complementary insurance as the universal coverage pays 100% of hospital but 75%(?) of other services so they purchase a private policy for additional coverage (perhaps one of our Australian peas can weigh in). I don't support a high deductible catastrophic plan simply because of what I personally went through. I've met my deductible & max OOP for four years now. I would be bankrupt if I had to pay $15,000 each year instead of the $4,000 I've had to pay. Private insurance that complements like Medicare Advantage, etc would be fine. But you have to offset the difference in premium. If you're currently paying a premium of $12,000 a year for a $4,000 deductible - your total expenditure is $16,000. The high deductible plan would have lower premiums - significantly - so you may be paying a premium of $1,000 with a $15,000 deductible (that's a crazy high deductible for an individual) so your total expenditure is the same. In comparing pricing for current plans in the market today - your total max out of pocket annually is lowest for a high deductible plan. We price compared them this year and the reduction in premiums is greater than the increase in deductibles. |
|
bbchangeup
Shy Member

Posts: 38 
|
Post by bbchangeup on Sept 29, 2017 15:21:23 GMT
There are many people who bristle at the way DoD handles healthcare but they are very good at it. They push you like MAD to make healthy choices, to eat right, to exercise, to prevent disease because when the system is paying for you cradle to grave, the incentive is there to keep you from getting sick in the first place. There is no profit for DoD in treating diabetes with expensive meds. They don't want to pay for that so the best way to keep from paying is not denying coverage but by making sure you never get diabetes in the first place. They won't pay for weight loss surgery until you've made the proper effort on your own to eat a healthier diet and exercise. THIS is the elephant in the room. I am continually amazed that we Americans feel that health care is a "right" yet we feel not one smidgen of responsibility for our own health. Some do -- not many. The vast majority of diseases of a chronic nature (heart disease, diabetes) are affected by our own choices. We want to make any choice we want, then bemoan the fact that someone won't pay to "fix it" and even after it's fixed, we want to continue the same behaviors that contributed to the condition in the first place. I teach public health at a Big Ten university. It has been apparent in the public health literature for decades that we need to get a grip on making ourselves responsible for our own health, and providing opportunities to do that. I started a thread once asking a simple question about how much responsibility the individual has for his/her own health. People brought up legitimate concerns - who decides what is caused by behavior, etc. Regardless, we are seeing increasing rates of obesity (especially childhood), rates of diabetes, rates of certain cancers - that are directly linked to behavior. That is where "the fix" needs to come from, or we can spend more and more on keeping people "insured" while we see no behavior changes that would result in better health AND less of our GDP being spent on health care. But we're not moving towards a society where personal responsibility is very easily accepted, so I don't think anything we do can really get at the root of the problem until we admit it - we need to eat less, exercise more, drink less, smoke less, and work every single day to make ourselves as healthy as we can - we hold the cards by accepting that personal responsibility. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:22:07 GMT
Are you seriously talking about nationalizing all of the hospitals, drug companies and medical equipment manufacturers? Nope. Just making them non-profit. There is no country in the world with that system and it is completely and totally impossible politically to propose in this country. This is rhetoric that does nothing to actually solve the health care issues in this country. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 15:31:16 GMT
Nope. Just making them non-profit. There is no country in the world with that system and it is completely and totally impossible politically to propose in this country. This is rhetoric that does nothing to actually solve the health care issues in this country. I. Disagree. Intelligent people of good will can find a way to take profit out of misery.They can start by regulating it as a utility and knocking down the double-digit profit margins of drug companies. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 15:45:42 GMT
 "n the U.S. health care system, everything costs more. Being in a hospital cost more. Because our drugs cost more (prescription drug prices can be 10X the rate in the UK or Germany). And our doctors cost more (a US family physician makes 3X her German counterpart). B ecause their education costs more (the education for a German physician's education is nearly free). And on it goes.... Near the end of the book, Reid expands on two big reasons why U.S. health care is so expensive: (1) Unlike other countries, the U.S. government doesn't manage prices; and (2) the complications created by our for-profit system adds tremendous costs. First, it really starts with the prices. While some developed countries have one health care insurance plan for everybody -- where the government either sets prices or oversees price negotiations -- the U.S. is unique in our reliance on for-profit insurance companies to pay for both essential and elective care. Twenty cents from every $1 goes, not to health care, but to "marketing, underwriting, administration, and profit," he says. In a system where government doesn't negotiate prices down, prices will be higher. In a system where for-profit companies need profit margins and advertising, prices will be higher." www.theatlantic.com/business/archive/2013/03/why-is-american-health-care-so-ridiculously-expensive/274425/ |
|
|
|
Post by Darcy Collins on Sept 29, 2017 15:47:22 GMT
There is no country in the world with that system and it is completely and totally impossible politically to propose in this country. This is rhetoric that does nothing to actually solve the health care issues in this country. I. Disagree. Intelligent people of good will can find a way to take profit out of misery.They can start by regulating it as a utility and knocking down the double-digit profit margins of drug companies. Good luck with that - you do realize 3 of the 5 biggest pharmaceutical companies aren't even US companies. But propose to make them non-profit and you can successfully drive out the other two. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 15:51:54 GMT
I. Disagree. Intelligent people of good will can find a way to take profit out of misery.They can start by regulating it as a utility and knocking down the double-digit profit margins of drug companies. - you do realize 3 of the 5 biggest pharmaceutical companies aren't even US companies. But propose to make them non-profit and you can successfully drive out the other two. Thanks! |
|
|
|
Post by compwalla on Sept 29, 2017 15:56:28 GMT
To get there in America, I think we need to allow people to buy into Medicare/Medicaid, especially in places where there is only one insurer in the marketplace. This is a version of the public option which I also agree is a good next step/big improvement to the ACA and where we should be going next. I am not married to any single idea other than universal coverage. If that ends up being single payer, yay. If it's a combination of public and private, yay. As long as we cover every American, however it ends up looking is fine with me. Allowing buy-in to Medicare seems like a doable next step. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 16:24:27 GMT
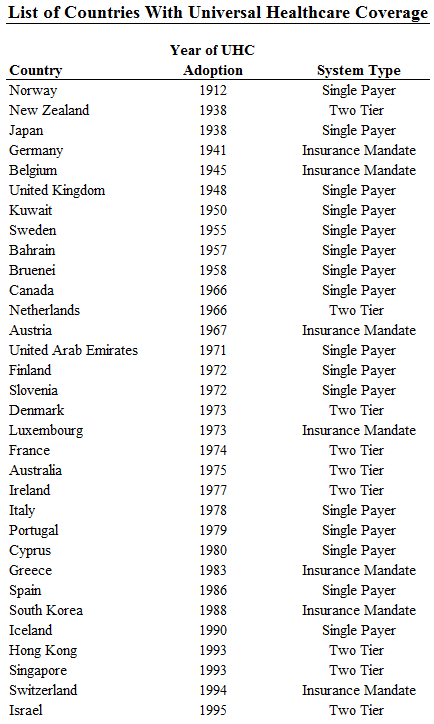
You need to understand single payer and universal health care are not the same thing at all. Stop using them interchangeably - it's just wrong. Germany does not have a single payer system by any stretch of the imagination - nor does Switzerland, or Japan etc etc. The number of single payer systems is actually quite small - and the number of single payer federal systems even smaller. Japan does have a single payer system and maybe more countries than you actually think there are. All those countries on that map do have Universal Health Care. The difference is not about the actual healthcare which is universal ( access to all citizens) it's about how it's funded that single payer comes into play. The UK's healthcare comes under single payer. Single Payer: The government provides insurance for all residents (or citizens) and pays all health care expenses except for copays and coinsurance. Providers may be public, private, or a combination of both.
Two-Tier: The government provides or mandates catastrophic or minimum insurance coverage for all residents (or citizens) while allowing the purchase of additional voluntary insurance or fee-for service care when desired. In Singapore all residents receive a catastrophic policy from the government coupled with a health savings account that they use to pay for routine care. In other countries like Ireland and Israel, the government provides a core policy which the majority of the population supplement with private insurance.
Insurance Mandate: The government mandates that all citizens purchase insurance, whether from private, public, or non-profit insurers. In some cases the insurer list is quite restrictive, while in others a healthy private market for insurance is simply regulated and standardized by the government. In this kind of system insurers are barred from rejecting sick individuals and individuals are required to purchase insurance, in order to prevent typical health care market failures from arising.
|
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 16:27:38 GMT
I keep seeing estimates of how much it will cost to insure people under a single payer system, and those costs are usually along with "this is xx much higher than the current budget." But wouldn't people be paying more money in to the government under a single payer system? The money that they are currently paying towards their premiums would be going towards the new insurance (hopefully at a much lower premium cost)? I'm not good with the numbers aspect so am genuinely asking a question. Not sure if I am missing something? That is it exactly. Instead of paying to the for-profit insurers, you would be paying more to a single admin system w/o profit - just like most developed countries have in some form or other. So, yes, your taxes would probably go up for some people and and your premiums would go away. And we'd get billions in duplicative admin costs, marketing costs, and profits out of the system. And you would be putting thousands of people out of work. What are you going to do about them? I just checked and as of 2015, just in the home offices of the carriers, it’s over 500,000. This is just health care carriers and it doesn’t include the employees out in the field. And those admin costs are shifted over to the government. You think the current system can handle 326M people? Again I’m not against a single payer system but if we move too fast we could really screw it up. |
|
|
|
Post by Darcy Collins on Sept 29, 2017 16:44:31 GMT
You need to understand single payer and universal health care are not the same thing at all. Stop using them interchangeably - it's just wrong. Germany does not have a single payer system by any stretch of the imagination - nor does Switzerland, or Japan etc etc. The number of single payer systems is actually quite small - and the number of single payer federal systems even smaller. Japan does have a single payer system and maybe more countries than you actually think there are. All those countries on that map do have Universal Health Care. The difference is not about the actual healthcare which is universal ( access to all citizens) it's about how it's funded that single payer comes into play. The UK's healthcare comes under single payer. Single Payer: The government provides insurance for all residents (or citizens) and pays all health care expenses except for copays and coinsurance. Providers may be public, private, or a combination of both.
Two-Tier: The government provides or mandates catastrophic or minimum insurance coverage for all residents (or citizens) while allowing the purchase of additional voluntary insurance or fee-for service care when desired. In Singapore all residents receive a catastrophic policy from the government coupled with a health savings account that they use to pay for routine care. In other countries like Ireland and Israel, the government provides a core policy which the majority of the population supplement with private insurance.
Insurance Mandate: The government mandates that all citizens purchase insurance, whether from private, public, or non-profit insurers. In some cases the insurer list is quite restrictive, while in others a healthy private market for insurance is simply regulated and standardized by the government. In this kind of system insurers are barred from rejecting sick individuals and individuals are required to purchase insurance, in order to prevent typical health care market failures from arising.
Japan's health care isn't single payer. There are 8 insurance systems with 3,500 insurers. I found that graph to be wholly inaccurate. Norway's system is managed on a municipality level - not federal; Canada's is by providence. The UK is one of the very few who has implemented a federal, single payer system. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 17:11:16 GMT
Japan's health care isn't single payer. There are 8 insurance systems with 3,500 insurers. I found that graph to be wholly inaccurate. Norway's system is managed on a municipality level - not federal; Canada's is by providence. The UK is one of the very few who has implemented a federal, single payer system. You'd better take it up with the WHO then. It came from one of several research papers in a series commissioned by the World Health Organization for the First Global Symposium on Health Systems Research. Norway is managed by four regional health care services but they are funded and overseen by the Ministry of Health and Care Services not much different to what it is in the UK. Maybe your definition of " single payer" isn't the same as anyone else's perhaps! |
|
|
|
Post by Darcy Collins on Sept 29, 2017 18:51:26 GMT
Japan's health care isn't single payer. There are 8 insurance systems with 3,500 insurers. I found that graph to be wholly inaccurate. Norway's system is managed on a municipality level - not federal; Canada's is by providence. The UK is one of the very few who has implemented a federal, single payer system. You'd better take it up with the WHO then. It came from one of several research papers in a series commissioned by the World Health Organization for the First Global Symposium on Health Systems Research. Norway is managed by four regional health care services but they are funded and overseen by the Ministry of Health and Care Services not much different to what it is in the UK. Maybe your definition of " single payer" isn't the same as anyone else's perhaps! You're ignoring the fact that it's the actual municipalities in Norway who are responsible for administration. In the context of this discussion, about whether a single national entity administrating the health care system for a country is the norm around the world - it doesn't qualify. I understand that the WHO is classifying based on whether it's governmental funded or not - but that's not what I was arguing. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 20:16:12 GMT
1. Medicaid is expanded to all states and individuals don’t have a choice if they buy insurance or not. 2. Democrats should mount a serious attempt to move people from low income to the middle class. I agree w/both points above. But how do we FUND THEM!?!?!?!?! With taxing the middle and poor more?  Or w/taxing the wealthiest more?!??! People keep ignoring that the vast majority of the money is locked up in the hands of a small minority of the households. So, if not from the richest, where do we get the money to get people off drugs, expand medicaid, pay for nursing home care, pay for law enforcement, clean water, safe food, cancer care and all the other ways we can help people's lives to be less miserable and more healthy, peaceful and productive? 1. The ACA has funding taxes built into it. This was one of the reasons the GOP wanted to repeal it. Anyway I believe when the ACA was set up they took into consideration all states would expand Medicaid. It wouldn’t have made any sense if they hadn’t. The big monkey wrench was all the sick people. And the number of people who took the fine instead of buying insurance. Both were underestimated IMO. Both are the crux of the problem. And both need to be dealt with. Along with getting Medicaid expanded in all states. 2. Surprising enough there are already programs to help workers retrain for other jobs. The junior college near me checks with local employers on what skills are needed and then sets up programs to teach the kids these skills. The framework is already there in a lot of areas. The problem, as I see it, too many workers think they don’t have to do anything about retraining or any training because it’s just a matter of time until those good jobs come back and they won’t require any additional training or retraining. They believe that because that is what the politicians are telling them. Pay attention to what trump and the GOP say when it comes to jobs. All they say is they are bringing back jobs. But yet employers are saying we have openings but can’t find skill workers to do the job. Or pass the drug tests. The last number released there were 6.2M job openings and roughly 7M people looking for work. IMO the Democrats need to start telling the American people the truth when it comes to jobs. They need to talk about it on the local level, on the state level, and on the federal level. Here is my three step plan to move more people from low income to middle class. 1. Convince people that a) certain jobs are gone and not coming back and more are likely to disappear b) as some jobs disappear new jobs will take their place that will require new training/skills. 2. Once people are convinced they are going to need certain skills then it’s up to not just the government (local, state & federal) but businesses and schools to put in place programs to train/retrain workers. 3. Once you have the skilled workers then it’s up to the local and state government to woo businesses to their area. Look at Elon Musk and his battery plant outside Reno. He went shopping for a deal. He got it and it is becoming a boom to the area. Amazon is shopping its 2nd headquarters. If it’s done right the deal could benefit both Amazon and the area where it’s built. But the key is that it must really be beneficial to both sides. Again IMO this should be the key to the Democrats platform and their main talking point. One of the reason trump won was because of jobs. People who voted for President Obama voted for trump because of jobs. It’s going to take time to convince people they need to change how they think about jobs. My biggest gripe against Hillary is when she started talking about a changing job market to the coal miners and they didn’t take it well so she backed off and didn’t talk about it again until after the election. Even if she had kept talking about it she may have still lost the election. But at least she would have been telling what the future job market will be even if the people weren’t ready to hear it. As far as programs go Like I said earlier I was surprised how many programs there are out there to help workers. Unfortunately I’m finding out about them because they are earmarked by trump/GOP to be eliminated to pay for their tax cuts. How to pay pay for this? As we push more people from low income to middle class the more tax money will come in to help fund the programs including health care. Close the tax loopholes the corporations and the wealthy take great delight in using. Look at the budget. Do we need all those subsidies? Can some be pared back or eliminated and transferred to programs that help the masses? Do we really need the big increase in funds to the military trump/GOP claim are needed. We already spend more on our military then any other country. Maybe instead of throwing money at the military we should look how its spent. Find better ways of allocating the money to give the milita4y what it needs without breaking the bank. None of this is easy. But just taxing the hell out of the rich isn’t the answer either. IMO |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 29, 2017 21:48:12 GMT
I agree w/both points above. But how do we FUND THEM!?!?!?!?! With taxing the middle and poor more? Or w/taxing the wealthiest more?!??! People keep ignoring that the vast majority of the money is locked up in the hands of a small minority of the households. So, if not from the richest, where do we get the money to get people off drugs, expand medicaid, pay for nursing home care, pay for law enforcement, clean water, safe food, cancer care and all the other ways we can help people's lives to be less miserable and more healthy, peaceful and productive? 1. The ACA has funding taxes built into it. This was one of the reasons the GOP wanted to repeal it. Anyway I believe when the ACA was set up they took into consideration all states would expand Medicaid. It wouldn’t have made any sense if they hadn’t. The big monkey wrench was all the sick people. And the number of people who took the fine instead of buying insurance. Both were underestimated IMO. Both are the crux of the problem. And both need to be dealt with. Along with getting Medicaid expanded in all states. 2. Surprising enough there are already programs to help workers retrain for other jobs. The junior college near me checks with local employers on what skills are needed and then sets up programs to teach the kids these skills. The framework is already there in a lot of areas. The problem, as I see it, too many workers think they don’t have to do anything about retraining or any training because it’s just a matter of time until those good jobs come back and they won’t require any additional training or retraining. They believe that because that is what the politicians are telling them. Pay attention to what trump and the GOP say when it comes to jobs. All they say is they are bringing back jobs. But yet employers are saying we have openings but can’t find skill workers to do the job. Or pass the drug tests. The last number released there were 6.2M job openings and roughly 7M people looking for work. IMO the Democrats need to start telling the American people the truth when it comes to jobs. They need to talk about it on the local level, on the state level, and on the federal level. Here is my three step plan to move more people from low income to middle class. 1. Convince people that a) certain jobs are gone and not coming back and more are likely to disappear b) as some jobs disappear new jobs will take their place that will require new training/skills. 2. Once people are convinced they are going to need certain skills then it’s up to not just the government (local, state & federal) but businesses and schools to put in place programs to train/retrain workers. 3. Once you have the skilled workers then it’s up to the local and state government to woo businesses to their area. Look at Elon Musk and his battery plant outside Reno. He went shopping for a deal. He got it and it is becoming a boom to the area. Amazon is shopping its 2nd headquarters. If it’s done right the deal could benefit both Amazon and the area where it’s built. But the key is that it must really be beneficial to both sides. Again IMO this should be the key to the Democrats platform and their main talking point. One of the reason trump won was because of jobs. People who voted for President Obama voted for trump because of jobs. It’s going to take time to convince people they need to change how they think about jobs. My biggest gripe against Hillary is when she started talking about a changing job market to the coal miners and they didn’t take it well so she backed off and didn’t talk about it again until after the election. Even if she had kept talking about it she may have still lost the election. But at least she would have been telling what the future job market will be even if the people weren’t ready to hear it. As far as programs go Like I said earlier I was surprised how many programs there are out there to help workers. Unfortunately I’m finding out about them because they are earmarked by trump/GOP to be eliminated to pay for their tax cuts. How to pay pay for this? As we push more people from low income to middle class the more tax money will come in to help fund the programs including health care. Close the tax loopholes the corporations and the wealthy take great delight in using. Look at the budget. Do we need all those subsidies? Can some be pared back or eliminated and transferred to programs that help the masses? Do we really need the big increase in funds to the military trump/GOP claim are needed. We already spend more on our military then any other country. Maybe instead of throwing money at the military we should look how its spent. Find better ways of allocating the money to give the milita4y what it needs without breaking the bank. None of this is easy. But just taxing the hell out of the rich isn’t the answer either. IMO Very well thought out. I mostly agree with you. But I still think it is obscene for 10% of the population to hold 76% of the wealth. We need to tax the wealthy much more aggressively in my opinion. We can't keep looking to the middle to save this country when 90% of us only own 24% of the wealth |
|
|
|
Post by *leslie* on Sept 29, 2017 22:15:07 GMT
I'm curious what happens in government run healthcare with doctors, nurses or any other health care professional? If they don't want to be a government employee, what do they do?
|
|
|
|
Post by 950nancy on Sept 29, 2017 22:34:22 GMT
We just received our new rates for 2018. Mine is going up $40 (as will my husband's). My son's is doubling since he is going in the grownup's age bracket. It could have been much worse, but our deductible is HUGE. We do have insurance for accidents though that covers that deductible.
|
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 30, 2017 0:05:49 GMT
You'd better take it up with the WHO then. It came from one of several research papers in a series commissioned by the World Health Organization for the First Global Symposium on Health Systems Research. Norway is managed by four regional health care services but they are funded and overseen by the Ministry of Health and Care Services not much different to what it is in the UK. Maybe your definition of " single payer" isn't the same as anyone else's perhaps! You're ignoring the fact that it's the actual municipalities in Norway who are responsible for administration. In the context of this discussion, about whether a single national entity administrating the health care system for a country is the norm around the world - it doesn't qualify. I understand that the WHO is classifying based on whether it's governmental funded or not - but that's not what I was arguing. If that's your argument then you are also ignoring the fact that the UK has the same system of administration as Norway and yet you're saying that the UK is one of the very few who has implemented a federal, single payer system. Both systems are the same. Norway's healthcare is administered and run by four municipalities and funded and overseen by their government. The UK is also administered by four municipalities....England.Scotland, Wales and Northern Ireland, funded and overseen by the government. And yet you differentiate between the two. I don't understand what exactly is it you are arguing about. A single payer healthcare is exactly what it says it is...it's totally government funded. Who and how many municipalities that is responsible for the performance or management of the healthcare to their citizens is irrelevant, it is still a single payer system that is totally funded by the government of that particular country. |
|
|
|
Post by Darcy Collins on Sept 30, 2017 1:11:09 GMT
You're ignoring the fact that it's the actual municipalities in Norway who are responsible for administration. In the context of this discussion, about whether a single national entity administrating the health care system for a country is the norm around the world - it doesn't qualify. I understand that the WHO is classifying based on whether it's governmental funded or not - but that's not what I was arguing. If that's your argument then you are also ignoring the fact that the UK has the same system of administration as Norway and yet you're saying that the UK is one of the very few who has implemented a federal, single payer system. Both systems are the same. Norway's healthcare is administered and run by four municipalities and funded and overseen by their government. The UK is also administered by four municipalities....England.Scotland, Wales and Northern Ireland, funded and overseen by the government. And yet you differentiate between the two. I don't understand what exactly is it you are arguing about. A single payer healthcare is exactly what it says it is...it's totally government funded. Who and how many municipalities that is responsible for the performance or management of the healthcare to their citizens is irrelevant, it is still a single payer system that is totally funded by the government of that particular country. It's not just 4 - Norway has 428 municipalities. Right now the US is debating whether a central or decentralized system is prudent - in addition to about a million other things. Looking at whether countries use a centralized system is utterly relevant to us. Funding is a separate issue - that is also relevant as we're considering how to fix our health care system. |
|
Deleted
Posts: 0
Jun 18, 2024 11:38:39 GMT
|
Post by Deleted on Sept 30, 2017 1:59:35 GMT
If that's your argument then you are also ignoring the fact that the UK has the same system of administration as Norway and yet you're saying that the UK is one of the very few who has implemented a federal, single payer system. Both systems are the same. Norway's healthcare is administered and run by four municipalities and funded and overseen by their government. The UK is also administered by four municipalities....England.Scotland, Wales and Northern Ireland, funded and overseen by the government. And yet you differentiate between the two. I don't understand what exactly is it you are arguing about. A single payer healthcare is exactly what it says it is...it's totally government funded. Who and how many municipalities that is responsible for the performance or management of the healthcare to their citizens is irrelevant, it is still a single payer system that is totally funded by the government of that particular country. Right now the US is debating whether a central or decentralized system is prudent - in addition to about a million other things. Looking at whether countries use a centralized system is utterly relevant to us. Funding is a separate issue - that is also relevant as we're considering how to fix our health care system. You called them municipalities when you were disputing what I originally said on who administrated their healthcare You said... My answer to that was: Then you carried on calling the administration of their healthcare by municipality
....call them what you like, municipalities/regions/districts whatever, they only have four of them administrating their healthcare. Norway has four designated Regional Health Authorities. They are: Northern Norway Regional Health Authority, Central Norway Regional Health Authority, Western Norway Regional Health Authority, and Southern and Eastern Norway Regional Health Authority.While some of the responsibility in the delivery has been decentralized to local authorities it is still financed by taxation therefore classed as a single payer system. ETA - Isn't this what you called out @zingermack for, to make the distinction between Universal Health care ( the delivery ) and single payer ( the funding) for. I was disagreeing with you only about the classification of funding for Norway. |
|









 Or w/taxing the wealthiest more?!??! People keep ignoring that the vast majority of the money is locked up in the hands of a small minority of the households.
Or w/taxing the wealthiest more?!??! People keep ignoring that the vast majority of the money is locked up in the hands of a small minority of the households. 

