Deleted
Posts: 0
Aug 18, 2025 20:12:27 GMT
|
Post by Deleted on Mar 31, 2016 15:22:31 GMT
justkat I wish I could like that post x1000. The 10/10 pain thing is really bugging me lately. EVERYONE thinks their pain is a 10 and I know this stuff is subjective but when you say that and you have no other clinical symptoms and you are walking and talking and eating everything in sight, I have a hard time believing you. Now, the guy with an open knee cap fracture or bilateral forearm fractures, or the guy with a dehissed wound post knee replacement and the hardware is sticking out and there is about 2-3 units of his blood in the floor....THAT guy is a 10. Funny, the knee replacement guy said, "nah, I'd say I'm about a 3, 3.5." He looked like crap and his BP was like 70/shitty, HR 130. I was like, "Dude. You are totally a 10!" Other things we don't want to hear: "I've been out of my meds and need a refill. I'm out of my percocet, my phenergan, oh and my soma." "I've been out of my psych meds for about 2-3 weeks." "I'm allergic to norco, percocet, fentanyl, dilaudid, zofran, reglan, compazine..." Yeah, I'll bet you are. Or when we ask about the pt's medical history and they say "Nothing" but their med list populates.... Imdur, plavix, amiodarone, lisinopril, HCTZ, metformin...... I beg to differ. Dilaudid almost killed my husband's mother. |
|
raindancer
Pearl Clutcher

Posts: 3,095 
|
Post by raindancer on Mar 31, 2016 15:29:28 GMT
What the hell difference does it make if he gets hives or starts violently vomiting? It makes him miserable There is a big difference. Lots of people vomit with narcotics, it's a side effect of the drug and not an allergy and you don't want to limit your analgesic options unless there is a true allergy. The difference is that with the vomiting side effect that the right anti-emetic may well prevent it. Vomiting is not life threatening. Anaphylaxis is. So yes a big difference, "feeling miserable" vs potentially dying. I had a certain narcotic at home with a bad tooth abscess and one tablet had me over the toilet vomiting for the next 4 hours. Several months later in hospital for something else they mentioned giving me that same drug again, so I just said "I vomited for 4 hours last time I had it" the anaesthetist then gave me an anti-emetic (I didn't even ask/care what it was) and I was totally fine, no nausea or vomiting at all. Just telling the truth and telling medical professionals what happens means they can make better decisions on if/how to give some drugs, there's no need to make thing up that just pisses people off...as you've clearly already discovered. Well next time you have a small bowel obstruction, we will see how you feel when someone insists on giving you a med that makes you puke, even when there are other options that work fine for you, and we will give you an anti-emetic and then say how we are sorry when it doesn't help you. In the mean time, we will try to remember that being violently ill when you have a small bowel obstruction and are a high risk for perforation, that it's not the meds that will kill you, just the reaction that might. This is why I have such a strong distaste for so many medical professionals. The complete lack of individualization is frustrating. People know their bodies. They really do. And chronically ill patients don't need people who think they know better causing them pain and suffering as some bizarre ego trip. A little compassion, actually listening to a person, and knowing their history can go a long way to helping them get well. In study after study patients who feel listened too heal faster, have lower readmission rates. I get that there are people who are a pain in the ass. I get that there are people who are seeking drugs. But frankly, until and unless they demonstrate that to you, you should treat them like they have a brain in their head. I'm not a nurse or a doctor, but I have a degree in public health and I have taken a fair share of classes next to doctors and nurses in the making. In addition my husband has been chronically ill for all 20 years of our marriage. You know who knows more about a specific disease than you? The mother or wife of someone suffering from that disease. I can almost promise you that after advocating for years and years for that person we love, that we know more about how they are impacted as an individual by the medical procedures and treatments. A respect of that knowledge would go a long way in making the experience better for everyone involved. |
|
|
|
Post by monklady123 on Mar 31, 2016 15:29:51 GMT
When a patients says to me 'I have a very high pain tolerance" - that mostly means I'm going to be running to the drug supply for them all shift long. Same with "I'm a very good patient". you know that their finger is going to be on the bell more than anyone else's. People who feel the need to prepare you by telling you how little trouble they are going be already know that's not true...but somehow they still think that by saying it, you won't notice their constant demands. The other times you know you're in for it is when your perfectly lovely, normal, rational patient of 5 minutes ago says "what are you going to do with that snake under my bed" or "I heard you talking about me and I won't drink that poison and I'm calling the police". Then you know your well planned & organised shift is going straight to hell and you'll be making phone calls and getting sedative orders all night at best...at worse you'll be holding down an irrational. screaming patient who is trying to escape because everyone wants to kill her. Yes, I've seen a few of those.  Honestly, nurses are saints on earth. I remember one woman who seemed totally "with it" when she was admitted... I actually spoke to her not long after she came on the floor, she was fine.... Then suddenly she "flipped out" as my kids would say. She was sure that the devil was after her, so right away they called me as the chaplain. Since I know the best way to talk to someone about the devil there in the room.. ?  Well anyway, I was able to keep her occupied until they could get her to the "behavior unit" (i.e., psych). |
|
Deleted
Posts: 0
Aug 18, 2025 20:12:27 GMT
|
Post by Deleted on Mar 31, 2016 15:31:51 GMT
How about this patient doozy? "I can't stop throwing up. It is been constant all day." As said patient stands in front of me in full-glam make-up, eyes-poppin', lips smackin', hair perfectly in place, let's go out on a Saturday night. I don't know about you, but when *I* can't stop throwing up, I can barely brush my hair or go anywhere. But hey, to each their own, right? You met my friend Diane ! I had to take her the ER. And had to wait until she was READY! Because you never know how cute the doctor is going to be! And yes she did wrangle a date. |
|
|
|
Post by elaine on Mar 31, 2016 15:38:15 GMT
I have not had nearly as many pokes as her but the last one I had, the nurse tried a couple times and called for an anesthesiologist The trouble is that often when the nurse does believe the patient but the various doctors won't listen to the nurse. I admitted a lady one time who had been vomiting for several days, she was very overweight, had diabetes AND also told me that they always have trouble getting IVs in on her. So I called in the anaesthetist. He asked me how many times I'd tried and I said "none" then he proceeded to get shitty with me because I was calling him before I'd even tried. I pointed out all of the various reasons to him again and that I had looked at her arms carefully and couldn't even see enough to warrant a single attempt and said that I didn't think it was a good use of anyone's time or effort for me to stick her several times when I already knew I wouldn't be able to get it and in the process might potentially ruin a vein that he could have got. He came down later still complaining...he was on his 5th attempt when my shift finished and I went home...so I didn't get the chance to give him the "I told you so" look. So sometimes it's attitudes like these from those who are more experienced that guilt some nurses into trying when they already know it's not going to be successful. The 'I didn't try" isn't something well accepted in nursing, and is treated as a weakness even when there's a very good reason for it. I think sometimes the 'system' forgets that there are real people at the end of every nurse "trying". I completely believe this happens. And since it does, there are valid reasons why patients try to talk to the nurse about issues with finding a vein. No one likes being stuck multiple times. So, maybe the issue for many nurses belongs in the "things you don't want to hear medical personnel say" thread - as in a physician telling you, the nurse, to try sticking the patient a number of times before calling him or her - rather than in the "things you don't want your patient to say" thread. If a nurse, like the OP, wants to threaten coming at my neck if I explain how I am a hard stick and where to best do it, it makes me want to give a swift punch to the throat back. If the issues are with the physicians, don't take it out on the patients. I know that is easier said than done, but the attitude in the OP directed towards patients in those instances is uncalled for. |
|
|
|
Post by mcscrapper on Apr 2, 2016 1:58:04 GMT
I have a new one to add today.... Got a pt with a port-a-cath. We deal with these all the time. We ask what type it is and the wife says its a port. Yes, we know. What we would really like to know is if it is a power port or a "regular" port. I start feeling around at the port and it is not a power port. No biggie. I can stick that, too. I tell the primary nurse that is a regular port and I'll go get the supplies. The wife then proceeds to call their doc's office in Vanderbilt to "make sure we know what we are doing." She also states that she has "the numbing cream," and we tell her that it takes approx 45 minutes for that to work. This pt is pretty sick. We offer to stick him with a regular IV but they refuse that so we are back to the port. I understand that you don't know us but I just confirmed with another nurse that what kind of port we are dealing with and we deal with them all the time. We explain the differences between ports and I think she finally gets it. I come back with all the supplies and proceed to get myself sterile - mask, gloves, sterile field. I even tell the patient what's up. He's cool. The wife has the Vandy nurse on the phone and grabs my hands and tells me she wants me to talk to the nurse. The primary nurse assures the wife I know what I'm doing. I proceed to put on another set of gloves and the wife is still talking. I go ahead and a stick the pt and get the blood I need. The wife finally hangs up and tells us that we need a "hoover needle." The primary nurse tells her it is a "Huber needle and Meredith already stuck and got all the blood we need." I just wish people would let us do our jobs w/out trying to tell us how to do it all the time. We are a HUGE hospital - one of the largest in the country. We aren't some po-dunk, backwoods medical tent! sheesh! I truly get what y'all are saying about difficult IV sticks. What I have heartburn about is when a pt starts off saying, "You aren't gonna be able to get a vein on me. I'm a hard stick." 9/10 when people say that, I can get them on the first try...and I have to at least try twice before I can call call the "IV team." And I have never once stuck for blood with anything besides a butterfly needle. What other kinds of veinipuncture needles does the rest of the world use? m |
|
|
|
Post by pjaye on Apr 2, 2016 2:20:18 GMT
What other kinds of veinipuncture needles does the rest of the world use? I haven't been working in an environment where I take blood for a couple of years now and prior to that I worked in an ICU, so I've mostly taken art line bloods myself. However I think the most common equipment used here is the vacutainer system LINK. Most places I have worked have phlebotomists now (ward nurses don't routinely take blood anymore) and they all seem to use vacutainers from what I've seen. |
|
|
|
Post by Zee on Apr 2, 2016 2:31:29 GMT
There is a big difference. Lots of people vomit with narcotics, it's a side effect of the drug and not an allergy and you don't want to limit your analgesic options unless there is a true allergy. The difference is that with the vomiting side effect that the right anti-emetic may well prevent it. Vomiting is not life threatening. Anaphylaxis is. So yes a big difference, "feeling miserable" vs potentially dying. I had a certain narcotic at home with a bad tooth abscess and one tablet had me over the toilet vomiting for the next 4 hours. Several months later in hospital for something else they mentioned giving me that same drug again, so I just said "I vomited for 4 hours last time I had it" the anaesthetist then gave me an anti-emetic (I didn't even ask/care what it was) and I was totally fine, no nausea or vomiting at all. Just telling the truth and telling medical professionals what happens means they can make better decisions on if/how to give some drugs, there's no need to make thing up that just pisses people off...as you've clearly already discovered. Well next time you have a small bowel obstruction, we will see how you feel when someone insists on giving you a med that makes you puke, even when there are other options that work fine for you, and we will give you an anti-emetic and then say how we are sorry when it doesn't help you. In the mean time, we will try to remember that being violently ill when you have a small bowel obstruction and are a high risk for perforation, that it's not the meds that will kill you, just the reaction that might. This is why I have such a strong distaste for so many medical professionals. The complete lack of individualization is frustrating. People know their bodies. They really do. And chronically ill patients don't need people who think they know better causing them pain and suffering as some bizarre ego trip. A little compassion, actually listening to a person, and knowing their history can go a long way to helping them get well. In study after study patients who feel listened too heal faster, have lower readmission rates. I get that there are people who are a pain in the ass. I get that there are people who are seeking drugs. But frankly, until and unless they demonstrate that to you, you should treat them like they have a brain in their head. I'm not a nurse or a doctor, but I have a degree in public health and I have taken a fair share of classes next to doctors and nurses in the making. In addition my husband has been chronically ill for all 20 years of our marriage. You know who knows more about a specific disease than you? The mother or wife of someone suffering from that disease. I can almost promise you that after advocating for years and years for that person we love, that we know more about how they are impacted as an individual by the medical procedures and treatments. A respect of that knowledge would go a long way in making the experience better for everyone involved. You are absolutely right that you and your DH know his body and his history much better than I do, and I respect that. If you told me no demerol because of severe nausea/vomiting, I will make sure you get something else. No need to lie. And I'm never afraid to admit when a patient is better-informed about something I'm unfamiliar with. Honesty is the best policy and I find patients and their families appreciate the respect I give them and usually are in turn more respectful if I DO know more than they do about something else. But the difference between nausea and hives actually IS significant. It's the difference between needing anti-nausea medication vs potential anaphylaxis. That's stuff we need to know. |
|
|
|
Post by mcscrapper on Apr 2, 2016 2:32:25 GMT
What other kinds of veinipuncture needles does the rest of the world use? I haven't been working in an environment where I take blood for a couple of years now and prior to that I worked in an ICU, so I've mostly taken art line bloods myself. However I think the most common equipment used here is the vacutainer system LINK. Most places I have worked have phlebotomists now (ward nurses don't routinely take blood anymore) and they all seem to use vacutainers from what I've seen. I get that. What I mean is for a straight up needle-to-vein blood draw, I've only ever used a butterfly needle but some people are saying that a different type of needle is used. I am just wondering what kind of needle they are using. I have a b'fly with a thin tube on it with the vaccutainer needle on the other end. We attach an access device to the end of that just for ease of putting the tubes on the vaccutainer. make sense? m |
|
|
|
Post by freecharlie on Apr 2, 2016 2:40:03 GMT
justkat I wish I could like that post x1000. The 10/10 pain thing is really bugging me lately. EVERYONE thinks their pain is a 10 and I know this stuff is subjective but when you say that and you have no other clinical symptoms and you are walking and talking and eating everything in sight, I have a hard time believing you. Now, the guy with an open knee cap fracture or bilateral forearm fractures, or the guy with a dehissed wound post knee replacement and the hardware is sticking out and there is about 2-3 units of his blood in the floor....THAT guy is a 10. Funny, the knee replacement guy said, "nah, I'd say I'm about a 3, 3.5." He looked like crap and his BP was like 70/shitty, HR 130. I was like, "Dude. You are totally a 10!" Other things we don't want to hear: "I've been out of my meds and need a refill. I'm out of my percocet, my phenergan, oh and my soma." "I've been out of my psych meds for about 2-3 weeks." "I'm allergic to norco, percocet, fentanyl, dilaudid, zofran, reglan, compazine..." Yeah, I'll bet you are. Or when we ask about the pt's medical history and they say "Nothing" but their med list populates.... Imdur, plavix, amiodarone, lisinopril, HCTZ, metformin...... I beg to differ. Why does that bother you? Guess what I am allergic to reglan, morphine, vanco (red mans syndrome), demerol, stadol, codine, and every other pain main underbthe sun that is a narc. I can take regular tylenol and regular motrin (max 800mg). my guess is typically the patient ot slooking for some particular pain drug to sell or abuse |
|
|
|
Post by Zee on Apr 2, 2016 2:42:32 GMT
I have a new one to add today.... Got a pt with a port-a-cath. We deal with these all the time. We ask what type it is and the wife says its a port. Yes, we know. What we would really like to know is if it is a power port or a "regular" port. I start feeling around at the port and it is not a power port. No biggie. I can stick that, too. I tell the primary nurse that is a regular port and I'll go get the supplies. The wife then proceeds to call their doc's office in Vanderbilt to "make sure we know what we are doing." She also states that she has "the numbing cream," and we tell her that it takes approx 45 minutes for that to work. This pt is pretty sick. We offer to stick him with a regular IV but they refuse that so we are back to the port. I understand that you don't know us but I just confirmed with another nurse that what kind of port we are dealing with and we deal with them all the time. We explain the differences between ports and I think she finally gets it. I come back with all the supplies and proceed to get myself sterile - mask, gloves, sterile field. I even tell the patient what's up. He's cool. The wife has the Vandy nurse on the phone and grabs my hands and tells me she wants me to talk to the nurse. The primary nurse assures the wife I know what I'm doing. I proceed to put on another set of gloves and the wife is still talking. I go ahead and a stick the pt and get the blood I need. The wife finally hangs up and tells us that we need a "hoover needle." The primary nurse tells her it is a "Huber needle and Meredith already stuck and got all the blood we need." I just wish people would let us do our jobs w/out trying to tell us how to do it all the time. We are a HUGE hospital - one of the largest in the country. We aren't some po-dunk, backwoods medical tent! sheesh! I truly get what y'all are saying about difficult IV sticks. What I have heartburn about is when a pt starts off saying, "You aren't gonna be able to get a vein on me. I'm a hard stick." 9/10 when people say that, I can get them on the first try...and I have to at least try twice before I can call call the "IV team." And I have never once stuck for blood with anything besides a butterfly needle. What other kinds of veinipuncture needles does the rest of the world use? m She's probably been taught that targeting that port is a very specialized procedure and NOT to let just anyone at it with any old needle. Where I used to work we had a specific protocol for targeting ports. Not everyone was allowed, for good reason--some ports got fucked up by nurses thinking they know their jobs. I don't know where you are but butterfly needles are the exception rather than the rule at every place I've worked, whether it was a phleb or a nurse drawing. I'm in an office now and draw blood every day. I use this type most often, though a butterfly set can also be used with the vacutainer holder. I only use that for really tiny veins or those nervous Nellies who think that that's the only kind that can be used upon them, no matter the actual size or condition of their veins  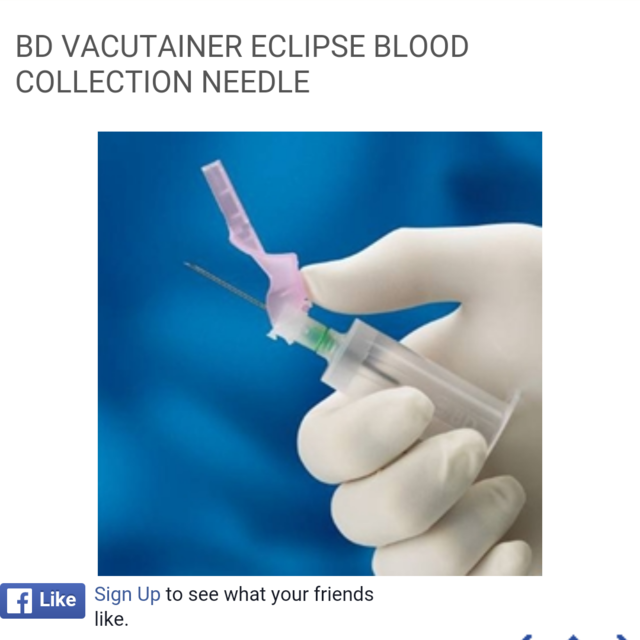 |
|
|
|
Post by Zee on Apr 2, 2016 2:45:00 GMT
Why does that bother you? Guess what I am allergic to reglan, morphine, vanco (red mans syndrome), demerol, stadol, codine, and every other pain main underbthe sun that is a narc. I can take regular tylenol and regular motrin (max 800mg). my guess is typically the patient ot slooking for some particular pain drug to sell or abuse Yeah, I most often heard "I am allergic to morphine, Tylenol, Percocet, vicodin, codeine, everything except dilaudid...I think...whatever is the strongest one, my doctor said that's the only kind I can have" Lolol |
|
|
|
Post by pjaye on Apr 2, 2016 2:46:15 GMT
I get that. What I mean is for a straight up needle-to-vein blood draw,
That's what I answered. Did you go to the link? It shows you exactly what it looks like and the needle on it.
Not sure how that can be misinterpreted, the pictures of the needle are pretty clear.
All of the vacutainers I have seen...come with that "normal" (for want of a better word) needle.
Normal/long 21G or 23G needles (not exactly sure which one, but I assume either of those sizes).
I have never seen a butterfly used with that system, I have never used a butterfly myself and I have never had a phlebotomist take blood with a butterfly either.
Clear now?
ETA: exactly what ZG posted.
|
|
|
|
Post by elaine on Apr 2, 2016 2:49:00 GMT
I have a new one to add today.... Got a pt with a port-a-cath. We deal with these all the time. We ask what type it is and the wife says its a port. Yes, we know. What we would really like to know is if it is a power port or a "regular" port. I start feeling around at the port and it is not a power port. No biggie. I can stick that, too. I tell the primary nurse that is a regular port and I'll go get the supplies. The wife then proceeds to call their doc's office in Vanderbilt to "make sure we know what we are doing." She also states that she has "the numbing cream," and we tell her that it takes approx 45 minutes for that to work. This pt is pretty sick. We offer to stick him with a regular IV but they refuse that so we are back to the port. I understand that you don't know us but I just confirmed with another nurse that what kind of port we are dealing with and we deal with them all the time. We explain the differences between ports and I think she finally gets it. I come back with all the supplies and proceed to get myself sterile - mask, gloves, sterile field. I even tell the patient what's up. He's cool. The wife has the Vandy nurse on the phone and grabs my hands and tells me she wants me to talk to the nurse. The primary nurse assures the wife I know what I'm doing. I proceed to put on another set of gloves and the wife is still talking. I go ahead and a stick the pt and get the blood I need. The wife finally hangs up and tells us that we need a "hoover needle." The primary nurse tells her it is a "Huber needle and Meredith already stuck and got all the blood we need." I just wish people would let us do our jobs w/out trying to tell us how to do it all the time. We are a HUGE hospital - one of the largest in the country. We aren't some po-dunk, backwoods medical tent! sheesh! I truly get what y'all are saying about difficult IV sticks. What I have heartburn about is when a pt starts off saying, "You aren't gonna be able to get a vein on me. I'm a hard stick." 9/10 when people say that, I can get them on the first try...and I have to at least try twice before I can call call the "IV team." And I have never once stuck for blood with anything besides a butterfly needle. What other kinds of veinipuncture needles does the rest of the world use? m You know what - when you see people in an ER, especially when they need an IV or a blood draw, you are in a position of power and they are at your mercy. You hold the needle. They are going to be stuck with it. Many/most people have had more than one painful experience related to a medical professional trying to put in an IV or draw blood. Many people in positions of less power and in potentially painful situations ARE understandably going to say something that apparently is going to annoy the snot out of you. A course in empathy and patient relations may be helpful for you - or maybe a viewing or 12 of the William Hurt film "The Doctor." I can say that a good portion of what you have said here is what I want to add to the "Things you don't want to hear your medical personnel say" thread. |
|
|
|
Post by lisacharlotte on Apr 2, 2016 2:55:29 GMT
I get blood drawn at a military hospital and they use the vacutainer shown above, no butterflies.
And yes I do have a high pain tolerance, no that doesn't mean I'm calling nurses for drugs. I never use anything more than ibuprofen or acetaminophen.
|
|
Deleted
Posts: 0
Aug 18, 2025 20:12:27 GMT
|
Post by Deleted on Apr 2, 2016 2:58:35 GMT
I haven't been working in an environment where I take blood for a couple of years now and prior to that I worked in an ICU, so I've mostly taken art line bloods myself. However I think the most common equipment used here is the vacutainer system LINK. Most places I have worked have phlebotomists now (ward nurses don't routinely take blood anymore) and they all seem to use vacutainers from what I've seen. I get that. What I mean is for a straight up needle-to-vein blood draw, I've only ever used a butterfly needle but some people are saying that a different type of needle is used. I am just wondering what kind of needle they are using. I have a b'fly with a thin tube on it with the vaccutainer needle on the other end. We attach an access device to the end of that just for ease of putting the tubes on the vaccutainer. make sense? m I don't know anything about different types of needles, but until my DD (Med Asst) educated me to the existence of the butterfly a couple of years ago, all I know is that a bigger needle was used. And it would hurt like a son of a bitch when the tubes would get swapped out. I always wound up with a 4" long bruise on the inside of my elbow from the 'regular' needles. I have to specifically request a butterfly needle every time I have blood drawn or else they will use the standard larger needle (about 2" long, I think. I try not to look). When I was in labor with my first and the nurse went to take blood, she cheerfully informed me that they'd run out of all the small and regular needles so she was going to be sticking me with the largest sized needles they had. OMG. That freaking HURT. When she took it out, blood spurted every freaking where. Thirty-two years later, I still have a scar from that blood draw. :mad So, all that to say that - in my experience - you have to specifically ask for a butterfly. L ETA: DH bruises pretty badly from blood draws, too. While he has no fear of needles, I once suggested that he ask for a butterfly for a blood draw. He loved it. It was virtually painless and he didn't bruise. He was happy about that. The next time he needed blood drawn and asked for the butterfly, the nurse refused. She said that the narrow channel in the BF needle caused blood cells to burst, rendering less-than-accurate lab results. Is there any truth to that? |
|
|
|
Post by pjaye on Apr 2, 2016 3:10:58 GMT
Many people in positions of less power and in potentially painful situations ARE understandably going to say something that apparently is going to annoy the snot out of you. A course in empathy and patient relations may be helpful for you - or maybe a viewing or 12 of the William Hurt film "The Doctor." That film was total rubbish. I'd venture to say that almost never happens. I've worked with lots a-hole doctors and a few of them had major health crisis themselves - bowel cancer (he had the chemo pump in his pocket and kept working), sudden cardiac arrest & ended up ventilated in another country etc...and you know what? They were exactly the same after their health crisis as before. I think this is just a vent/frustration post...but these things never go down well unless everyone else is a medical professional as well. When non medical people read it, they see it in a totally different light and therefore it attracts undue criticism. I might say after the event "I'll stick you where the sun don't shine" BUT at the time, I'll be standing there calmly with a nice smile on my face saying "I promise I'll be as gentle as I can". I get the need to vent, medical professional or not,dealing with the general public is hard anyway (and you'd be surprised how dumb a lot of people are about things that would seem to be basic knowledge), factor in sickness and fear and it's a tough gig...honestly you get treated like crap, you get told what to do you get abused on a regular basis for just doing your job. Sometimes you just need to blow off some steam about it all. But it's probably better to do it when there are only other medical professionals around...on a public message board, it's pretty well guaranteed to end in a shit storm. |
|
|
|
Post by pjaye on Apr 2, 2016 3:15:14 GMT
She said that the narrow channel in the BF needle caused blood cells to burst, rendering less-than-accurate lab results. Is there any truth to that? Not always but yes it can happen when smaller gauge needles are used. I can also happen when it's a difficult blood draw and it takes to much effort to get the blood, the blood vessels burst or clot and the results can be affected or often cannot be tested at all and will need to be redone. |
|
|
|
Post by Zee on Apr 2, 2016 3:15:30 GMT
I get that. What I mean is for a straight up needle-to-vein blood draw, I've only ever used a butterfly needle but some people are saying that a different type of needle is used. I am just wondering what kind of needle they are using. I have a b'fly with a thin tube on it with the vaccutainer needle on the other end. We attach an access device to the end of that just for ease of putting the tubes on the vaccutainer. make sense? m I don't know anything about different types of needles, but until my DD (Med Asst) educated me to the existence of the butterfly a couple of years ago, all I know is that a bigger needle was used. And it would hurt like a son of a bitch when the tubes would get swapped out. I always wound up with a 4" long bruise on the inside of my elbow from the 'regular' needles. I have to specifically request a butterfly needle every time I have blood drawn or else they will use the standard larger needle (about 2" long, I think. I try not to look). When I was in labor with my first and the nurse went to take blood, she cheerfully informed me that they'd run out of all the small and regular needles so she was going to be sticking me with the largest sized needles they had. OMG. That freaking HURT. When she took it out, blood spurted every freaking where. Thirty-two years later, I still have a scar from that blood draw. :mad So, all that to say that - in my experience - you have to specifically ask for a butterfly. L ETA: DH bruises pretty badly from blood draws, too. While he has no fear of needles, I once suggested that he ask for a butterfly for a blood draw. He loved it. It was virtually painless and he didn't bruise. He was happy about that. The next time he needed blood drawn and asked for the butterfly, the nurse refused. She said that the narrow channel in the BF needle caused blood cells to burst, rendering less-than-accurate lab results. Is there any truth to that? No, she's wrong. They wouldn't make them for blood draws if they caused the blood cells to burst. It's slower, though. The needle is still larger than a blood cell and you can see the blood freely entering and exiting the tubing, not breaking up and clumping. It's true that some tests will be inaccurate if the blood cells are broken, but that is mainly why we have to use a needle instead of a finger stick for certain tests. Milking the finger can cause some of the cells to burst, causing (for example) a false high potassium reading. She was a dirty whoring liar, tell your DH I said so  |
|
|
|
Post by pjaye on Apr 2, 2016 3:19:17 GMT
She was a dirty whoring liar, tell your DH I said so
I don't agree, I've experienced it when I've had difficulty getting blood and used a small needle but sent it anyway and got a call back that it needed to be retaken.
They wouldn't make them for blood draws if they caused the blood cells to burst. It's slower, though Do they make butterfly needles specially for taking blood? I always thought they were to administer drugs or fluids in the short term, not for blood taking. |
|
|
|
Post by Zee on Apr 2, 2016 3:26:55 GMT
She was a dirty whoring liar, tell your DH I said so
I don't agree, I've experienced it when I've had difficulty getting blood and used a small needle but sent it anyway and got a call back that it needed to be retaken.
They wouldn't make them for blood draws if they caused the blood cells to burst. It's slower, though Do they make butterfly needles specially for taking blood? I always thought they were to administer drugs or fluids in the short term, not for blood taking. They're the same thing. The ones I have are marked "vacutainer blood collection set" but it says on the box they can be used for short-term infusions as well, up to two hours, and they're indistinguishable from the rate ones I saw used for IVs in the hospital. Honestly, we never used them on the floor, but occasionally would get someone transferred with one in place. ETA if you needed to redraw, it was because you had trouble with the vein, not because of the butterfly tubing itself. Think about the size/placement of needles in the NICU. The blood cells are still the same size in an infant and adult. I've never once had a sample drawn with a butterfly rejected. |
|
|
|
Post by elaine on Apr 2, 2016 3:29:29 GMT
Many people in positions of less power and in potentially painful situations ARE understandably going to say something that apparently is going to annoy the snot out of you. A course in empathy and patient relations may be helpful for you - or maybe a viewing or 12 of the William Hurt film "The Doctor." That film was total rubbish. I'd venture to say that almost never happens. I've worked with lots a-hole doctors and a few of them had major health crisis themselves - bowel cancer (he had the chemo pump in his pocket and kept working), sudden cardiac arrest & ended up ventilated in another country etc...and you know what? They were exactly the same after their health crisis as before. I think this is just a vent/frustration post...but these things never go down well unless everyone else is a medical professional as well. When non medical people read it, they see it in a totally different light and therefore it attracts undue criticism. I might say after the event "I'll stick you where the sun don't shine" BUT at the time, I'll be standing there calmly with a nice smile on my face saying "I promise I'll be as gentle as I can". I get the need to vent, medical professional or not,dealing with the general public is hard anyway (and you'd be surprised how dumb a lot of people are about things that would seem to be basic knowledge), factor in sickness and fear and it's a tough gig...honestly you get treated like crap, you get told what to do you get abused on a regular basis for just doing your job. Sometimes you just need to blow off some steam about it all. But it's probably better to do it when there are only other medical professionals around...on a public message board, it's pretty well guaranteed to end in a shit storm. I agree with your post except for the term "undue criticism." There IS a power imbalance, and when you vent about what patients say when they are anxious to a POPULATION OF PATIENTS, criticism of those comments is "warranted," rather than "undue," IMO. I have never abused a medical professional, ever. But I could list things that would make people's head spin in terms of what has been done and said to me in the past 18 months. And it pisses me off to no end to read someone whose job it is to help sick people bitch about it here, especially things that are PERFECTLY UNDERSTANDABLE- like comments regarding needle sticks for blood draws and IVs. And I stand by my comment that a nurse who feels the need to bitch about those comments in a place like here, where many of us or our spouses or our kids have serious health issues, needs to either 1) take a course in empathy and patient relations; and/or 2) find a new job. I am mental health professional and I never take posts where people talk negatively about their counsellors and/or psychologists personally. I never feel the need to start a spin-off thread to vent about my patients when people post negative experiences with their counsellors and therapists. And I would never, ever, vent about what my patients say to me here. Ever. If I felt the need to do so, I would stop being a psychologist, because clearly I wasn't a good fit for the career. My venting in a place like here would never ever in a million years be warranted, appropriate, or acceptable. I don't think it is remotely appropriate for nurses or physicians or anyone else in a position of power over their clients/patients to vent about it in public. |
|
|
|
Post by pjaye on Apr 2, 2016 3:37:17 GMT
I'm not saying that it happens routinely and you would never use them, but if you have difficulty and you are using a smaller needle then it can increase the risk of a haemolysed sample. To me that's not lying.
Plus there's personal preference and experience. I've always used a green needle and a 10ml syringe, and I was comfortable with it and got blood successfully 99% of the time. Having someone ask me to use a butterfly when it's not something I've ever done to take blood, then increases the chances of me buggering it up.
To me it makes sense that if any sort of technician has lots of experience and is successful at doing something a certain way...then I should let them do it their way...rather than insist on "my" way when I don't have the same experience. I'm not going to tell the plumber or the carpet layer how I think they should do their job.
|
|
|
|
Post by Zee on Apr 2, 2016 3:41:53 GMT
She's a liar if she says she can't because it ruins the sample, no exceptions. That's not truthful. But I was joking, really. If she really had that experience many times, I'd have to think it's her technique that needs revising. Once or twice is one thing; multiple times, it's her.
But really, if you can use a regular needle, you can use a butterfly. It's slower and more annoying to do it that way if their veins can take a regular needle but whether I'm the plumber or not, if a patient insists, I'll give it a whirl and do my best to honor their wishes. It's not surgery, I'm not going to mess anything major up.
|
|
|
|
Post by Zee on Apr 2, 2016 3:48:03 GMT
Ugghh, sorry I have to keep going back and editing. I think I need to get off here and go to bed!
Interesting insights from both positions here, as always.
|
|
theshyone
Pearl Clutcher
Posts: 3,458
|
Post by theshyone on Apr 2, 2016 3:50:42 GMT
My nightmare blood draws have existed my entire life but scarred me permanently after having septic shock after ICD complications and needing round the clock blood draws for testing. A lab tech would come to my room and get to try three different pokes, then could wait ten minutes and try again three times then try again three times. Total of nine pokes. Then had to leave and someone else would get their nine tries. Then an hour had to pass. I had blood draws requested every three hours but frequently the first draw wasn't complete by the time the next three hour draw was needed. A pic line was not an option due to infectious diseases saying it was a infection risk, I blew out several central lines. I was in agony and have horror flashbacks to this. Anesthesiologist S would use ultrasounds to try and find veins. Picture A is typical blood draw, either there or on hands, thumbs, toes, heels, webbing. Picture B is just easier.  |
|
|
|
Post by elaine on Apr 2, 2016 3:51:53 GMT
I'm not saying that it happens routinely and you would never use them, but if you have difficulty and you are using a smaller needle then it can increase the risk of a haemolysed sample. To me that's not lying. Plus there's personal preference and experience. I've always used a green needle and a 10ml syringe, and I was comfortable with it and got blood successfully 99% of the time. Having someone ask me to use a butterfly when it's not something I've ever done to take blood, then increases the chances of me buggering it up. To me it makes sense that if any sort of technician has lots of experience and is successful at doing something a certain way...then I should let them do it their way...rather than insist on "my" way when I don't have the same experience. I'm not going to tell the plumber or the carpet layer how I think they should do their job.But a plumber or a carpet layer isn't doing something TO YOUR BODY. That can physically hurt you. That can cause discomfort. That can result in bruises, or in one case of mine a hematoma from an IV. It is complete rubbish, to borrow your phrase, to compare talking to a nurse about blood draws and IVs on your or your loved ones' bodies to carpet laying and plumbing. |
|
|
|
Post by pjaye on Apr 2, 2016 3:55:33 GMT
I don't think it is remotely appropriate for nurses or physicians or anyone else in a position of power over their clients/patients to vent about it in public. You don't think it's appropriate and you don't do it. That's fine, that's your opinion & your choice. I happen to have a different one. Venting about what happened to you on your work day is understandable and does not mean everyone who does it needs to change careers...be that a nurse or a plumber. BUT everyone who bitches about their work day needs to expect that other people will come and bitch back about their attitude. That's what happens on a public message board. No one person gets to decide what is appropriate for everyone - I get to say what I think and you get the same opportunity. As for the "you can't complain about your job when people here are sick" that's just bullshit. I'm not married... so do I get the right to get all pissy about "you can't bitch about your husband because I don't have one"? or "you can't complain about your father because mine died"? Total narcissistic bullshit. The whole world is not about you. People are unwell, and yes that's awful for them and I can still have compassion...but that has nothing whatsoever to do with my asshole patient from a week ago who wanted me to make coffee for his 30 relatives after he had toe surgery. AS for the "every medical professional who vents about their patients needs to get a different job" - good luck with doing your own surgery and prescribing you own drugs, based on that suggestion they'll be about 10 doctors and a handful of nurses left in the world. |
|
|
|
Post by freecharlie on Apr 2, 2016 4:03:36 GMT
That film was total rubbish. I'd venture to say that almost never happens. I've worked with lots a-hole doctors and a few of them had major health crisis themselves - bowel cancer (he had the chemo pump in his pocket and kept working), sudden cardiac arrest & ended up ventilated in another country etc...and you know what? They were exactly the same after their health crisis as before. I think this is just a vent/frustration post...but these things never go down well unless everyone else is a medical professional as well. When non medical people read it, they see it in a totally different light and therefore it attracts undue criticism. I might say after the event "I'll stick you where the sun don't shine" BUT at the time, I'll be standing there calmly with a nice smile on my face saying "I promise I'll be as gentle as I can". I get the need to vent, medical professional or not,dealing with the general public is hard anyway (and you'd be surprised how dumb a lot of people are about things that would seem to be basic knowledge), factor in sickness and fear and it's a tough gig...honestly you get treated like crap, you get told what to do you get abused on a regular basis for just doing your job. Sometimes you just need to blow off some steam about it all. But it's probably better to do it when there are only other medical professionals around...on a public message board, it's pretty well guaranteed to end in a shit storm. I agree with your post except for the term "undue criticism." There IS a power imbalance, and when you vent about what patients say when they are anxious to a POPULATION OF PATIENTS, criticism of those comments is "warranted," rather than "undue," IMO. I have never abused a medical professional, ever. But I could list things that would make people's head spin in terms of what has been done and said to me in the past 18 months. And it pisses me off to no end to read someone whose job it is to help sick people bitch about it here, especially things that are PERFECTLY UNDERSTANDABLE- like comments regarding needle sticks for blood draws and IVs. And I stand by my comment that a nurse who feels the need to bitch about those comments in a place like here, where many of us or our spouses or our kids have serious health issues, needs to either 1) take a course in empathy and patient relations; and/or 2) find a new job. I am mental health professional and I never take posts where people talk negatively about their counsellors and/or psychologists personally. I never feel the need to start a spin-off thread to vent about my patients when people post negative experiences with their counsellors and therapists. And I would never, ever, vent about what my patients say to me here. Ever. If I felt the need to do so, I would stop being a psychologist, because clearly I wasn't a good fit for the career. My venting in a place like here would never ever in a million years be warranted, appropriate, or acceptable. I don't think it is remotely appropriate for nurses or physicians or anyone else in a position of power over their clients/patients to vent about it in public. why can't medical professionals vent or tell stories? The peas on this thread aren't using names, sates, hell even cities. The thread started for medical people to say what they dislike hearing, it wasn't started to see if we agreed with them or not. Venting is healthy. Commiserating with others who hear the same types of things from the same types of people is healthy. They wouldn't do it in front of the patient or family. |
|
|
|
Post by elaine on Apr 2, 2016 4:16:59 GMT
I don't think it is remotely appropriate for nurses or physicians or anyone else in a position of power over their clients/patients to vent about it in public. You don't think it's appropriate and you don't do it. That's fine, that's your opinion & your choice. I happen to have a different one. Venting about what happened to you on your work day is understandable and does not mean everyone who does it needs to change careers...be that a nurse or a plumber. BUT everyone who bitches about their work day needs to expect that other people will come and bitch back about their attitude. That's what happens on a public message board. No one person gets to decide what is appropriate for everyone - I get to say what I think and you get the same opportunity. As for the "you can't complain about your job when people here are sick" that's just bullshit. I'm not married... so do I get the right to get all pissy about "you can't bitch about your husband because I don't have one"? or "you can't complain about your father because mine died"? Total narcissistic bullshit. The whole world is not about you. People are unwell, and yes that's awful for them and I can still have compassion...but that has nothing whatsoever to do with my asshole patient from a week ago who wanted me to make coffee for his 30 relatives after he had toe surgery. AS for the "every medical professional who vents about their patients needs to get a different job" - good luck with doing your own surgery and prescribing you own drugs, based on that suggestion they'll be about 10 doctors and a handful of nurses left in the world. I'm willing to bet that none of my current eye doctors and surgeons vent on a public message board. You name the amount and I'll commit it. I never said that medical professionals couldn't vent. Never. Nice try at twisting my words. I said it wasn't appropriate HERE. A non-medical public message board. Reading comprehension is your friend. And if if you don't understand the issue of power differential between nurse and patient and how that is different from "I don't have a husband", you are really clueless. (I don't think you are, I think you are making stupid arguments that don't apply as a red herring). I have been VERY CLEAR about the power differential part of the equation in my beef with this thread and if you can't understand it, well, I'm sorry for you. And guess what, the whole world isn't about you and the OP and other nurses who want to vent on public message boards that have nothing to do with medicine. Talk about narcissism. You vent here about your patients and you will get warranted and deserved criticism back in return. You and other nurses can post whatever you like. Whatever you like. Whatever YOU find appropriate. And I will respond with what Imthink appropriate, and apparently others will too. Do you wonder why there are so many responses about why people DO talk to nurses about needles on this thread? If it was undue feedback, it would just be me, but person after person after person has responded. But you go ahead and try to make this all about me. |
|







 Honestly, nurses are saints on earth. I remember one woman who seemed totally "with it" when she was admitted... I actually spoke to her not long after she came on the floor, she was fine.... Then suddenly she "flipped out" as my kids would say. She was sure that the devil was after her, so right away they called me as the chaplain. Since I know the best way to talk to someone about the devil there in the room.. ?
Honestly, nurses are saints on earth. I remember one woman who seemed totally "with it" when she was admitted... I actually spoke to her not long after she came on the floor, she was fine.... Then suddenly she "flipped out" as my kids would say. She was sure that the devil was after her, so right away they called me as the chaplain. Since I know the best way to talk to someone about the devil there in the room.. ?  Well anyway, I was able to keep her occupied until they could get her to the "behavior unit" (i.e., psych).
Well anyway, I was able to keep her occupied until they could get her to the "behavior unit" (i.e., psych).